Athletes push their bodies to the limits, and the spine — the central pillar of strength and motion — often bears the brunt of that effort. From acute on-field trauma to overuse injuries that evolve silently, spine-related conditions can threaten both performance and long-term health. At an interventional pain management practice, early diagnosis, precise treatment, and safe return-to-play strategies are essential to helping athletes recover fully and prevent re-injury.
Acute Spine Injury: On-Field Assessment
An appropriate on-field evaluation begins with rapid yet structured assessment following the “ABCs” — airway, breathing, and circulation — before moving on to neurologic function. The examiner should quickly determine whether the athlete can move extremities voluntarily, assess for midline spinal tenderness, and look for signs of neurologic deficit such as numbness or weakness. Any complaint of neck or back pain following high-impact trauma must be treated as a potential spinal injury until proven otherwise.
When to Immobilize and Transfer
If the athlete reports neck pain, paresthesia, paralysis, or loss of consciousness, immediate cervical spine immobilization is necessary. A rigid cervical collar and long backboard should be used to prevent secondary injury. Transfer should only be performed by trained personnel using a log-roll technique while maintaining in-line stabilization. Even seemingly minor collisions can result in unstable fractures or ligamentous injury — making precautionary immobilization the safest approach until imaging rules out instability.
Diagnosing and Treating Lumbar Spondylitic Injuries
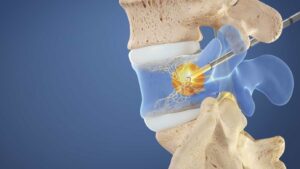
Chronic lumbar spondylitic injuries, including spondylolysis and spondylolisthesis, are common among athletes engaged in sports that require repetitive hyperextension, such as gymnastics, football, and diving. Diagnosis often requires MRI or CT imaging to identify pars interarticularis stress reactions or defects.
Treatment begins conservatively with activity modification, core-strengthening, and anti-inflammatory therapy. Interventional pain specialists may employ targeted epidural steroid injections, facet blocks, or radiofrequency ablation to manage inflammation and pain while rehabilitation progresses. Surgical referral becomes appropriate for high-grade slippage or persistent neurologic symptoms.
Return-to-Play Protocol
A structured return-to-play (RTP) protocol ensures safety and performance longevity. The athlete must achieve pain-free range of motion, full neurologic recovery, and core stability before resuming contact activities. Gradual progression from light aerobic exercise to sport-specific drills under medical supervision minimizes reinjury risk. Imaging confirmation of healing is often advised in cases of structural pathology such as spondylolysis or compression fractures.
Preventing Spine Injuries in Athletics
Prevention remains the most effective form of treatment. Coaches and sports medicine teams should emphasize neuromuscular training, flexibility, and postural awareness. Strengthening the paraspinal and abdominal muscles creates a natural brace for the spine, reducing mechanical stress. Proper technique — particularly in weightlifting and contact sports — plays a critical role in minimizing cumulative strain. Routine preseason screening can also identify at-risk athletes early, allowing for individualized conditioning programs.
Takeaway:
Spine-related injuries in athletes demand vigilance from the moment of impact through full recovery. A multidisciplinary approach that integrates on-field emergency care, diagnostic precision, interventional pain therapies, and guided rehabilitation not only restores function but also empowers athletes to return stronger — and safer — than before.