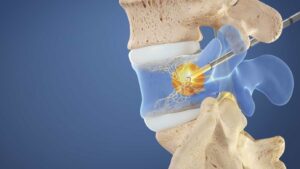
The use of steroids in interventional pain management procedures has transformed patient outcomes, enhancing both the quality and duration of pain relief. Steroids are known to decrease inflammation and swelling, and when used judicially, they can significantly alleviate pain. However, accurate dosing is imperative to maximize benefits and minimize potential risks, such as hormonal imbalance, infection, bleeding, or nerve damage. This article focuses on best practices and current evidence regarding steroid dosing for interventional pain management procedures.
Typically, steroid dosages range from 40mg to 80mg, depending on the type of procedure, severity of pain, and individual patient factors. For epidural steroid injections (ESIs), which are often used for radicular pain or spinal stenosis, the recommended dose of methylprednisolone acetate is 80mg, while triamcinolone acetonide is given at 40-60mg. Lumbar transforaminal epidural steroid injections typically utilize 40-80mg of triamcinolone.
However, patient characteristics and specific pain etiologies necessitate a personalized approach to dosing. For example, elderly patients or those with comorbidities such as diabetes or osteoporosis may require lower doses due to the potential for systemic steroid effects.
Research indicates that higher doses do not always correlate with better outcomes. A randomized trial comparing 80mg vs. 40mg of methylprednisolone in lumbar ESIs showed no significant difference in pain relief or function between the two doses at 3 weeks or 6 months post-injection. This suggests that a lower steroid dose may be as effective as a higher dose, with the added benefit of reduced potential for systemic effects.
Moreover, the selection of the steroid agent itself can influence the effectiveness and potential side effects. Particulate steroids such as triamcinolone or methylprednisolone have a higher risk of causing an infarct if accidentally injected intra-arterially, while non-particulate steroids like dexamethasone have a lower risk but might be less effective for prolonged pain relief.
The frequency of injections is another critical factor to consider. While repeat injections can provide continued pain relief, excessive use of steroids can lead to complications like weakening of the spinal bones or muscles and disruption of normal hormone production. The Spine Intervention Society suggests waiting at least two weeks between steroid injections and limiting to three to four injections per year.
In summary, steroid dosing for interventional pain management procedures requires a thorough understanding of patient characteristics, pain etiology, and current evidence to balance the benefits of pain relief with potential risks. A personalized, evidence-based approach to dosing, agent selection, and injection frequency can optimize outcomes and minimize adverse effects. Future research is needed to further refine steroid dosing guidelines and explore alternative agents that might provide similar benefits with fewer risks.