Neck pain can be caused by a variety of factors, mostly benign but some serious. A careful history, physical and appropriate diagnostic studies can help a doctor determine the diagnosis and plan an appropriate course of treatment that hopefully results in neck pain relief. You may find the use of a chiropractor to be helpful. If this is of interest of you then you may like to go to beachpaincenter.com.
A careful history should include questions pertaining to causative and related events such as infections, injury, stress or medications. The duration, nature of the pain, origin and associated symptoms such as weakness, numbness and tingling are important in determining a diagnosis. Alleviating or aggravating factors as well as surgical history are also important factors in determining the cause of the neck pain.
During physical examination to evaluate neck discomfort, your physician will first inspect your neck for any visual abnormalities. She/he will may then palpate the soft tissues and bony structures of your neck to check for signs of infection or other structural issues. Reproduction of neck pain with certain motions during the physical exam may assist your physician in determining a diagnosis. One example of this is the compression test, where your physician may press down on your head to reproduce the pain associated with nerve compression or a pinched nerve in your neck.
The anatomy of the neck, or cervical spine, is complex. It consists of seven cervical vertebrae (bones that provide structural support and house the spinal cord in the neck), eight cervical nerves that are derived from the spinal cord in the neck, inter-vertebral disks that lie between the vertebral bodies and act as a cushion, as well as joints that hold the vertebrae together and allow motion. These joints are lined by cartilage. Ligaments also help support the bony structure of the neck. The cervical nerves also divide into more nerves that innervate much of the head, the neck, the arms and other parts of the upper body. This elaborate structure and the complex signal processing mechanisms of the nerves, can be affected by numerous pathological states. In other words, there are numerous conditions that can cause neck or cervical spine pain.
One of the most common causes of neck pain is injury. This can result from an acute process such as an accident or repetitive stress and strain. Most neck pain causes are a result of such injuries or trauma. A very common neck injury is whiplash syndrome resulting from an automobile accident, especially a rear end collision. If this has happened to you then you can look into a whiplash settlement for a car accident here. Whiplash refers to the injury secondary to sudden hyperextension of the neck from an indirect force i.e. one not directly applied to the neck. Symptoms of whiplash injury may not occur for up to 24 hours after the injury because it may take this long for bleeding and swelling to develop as a response to the injury. About one in ten patients experience loss of consciousness and almost all patients develop neck pain and stiffness. The neck pain may radiate to the arms. A fair number also develop headaches and shoulder pain, or tennis elbow like symptoms.
Severe whiplash injury may result in damage to a cluster of nerves known as the cervical sympathetic chain, resulting in nausea, dizziness and ringing in the ears. Long term complications resulting from damage to the cervical sympathetic chain include a condition known as complex regional pain syndrome.
The diagnostic work up of neck trauma may involve X-rays to evaluate the cervical spine for bony damage and/or soft tissue injury. An MRI or a CT scan may be warranted for a more detailed diagnostic workup especially when symptoms persist or there are significant neurological symptoms. CT and MRI are more helpful than X-rays in evaluating soft tissues, disk abnormalities and nerve root compression, also called a “pinched nerve”. Electromyography is a diagnostic test that may be utilized to test for nerve compression/damage as well.
Myofascial pain syndrome is a common cause of chronic neck pain. It results in pain that is referred from trigger points, which are tender knots in the muscle. These trigger points restrict full lengthening of muscles and can weaken them. Pressing on a trigger point can cause pain at the site as well as in a referred pattern, i.e. pain away from the cause of the pain. They appear to results after an acute episode of muscle stress or strain. The muscle contracts, decreasing blood flow to the area. Nerve fibers connect the trigger point to the spinal cord and cause the pain to travel. Other symptoms such as sweating and erection of body hair, or piloerection, may also result. The pain is typically described as steady, deep and aching.
Myofascial pain can be exacerbated by viral illness, exposure to cold, strenuous exercise, typing, driving, carrying heavy shoulder bags and certain sleeping positions. This condition may coexist with other cervical spine disorders and can mimic these disorders as well, such as a herniated disk. Medical management of myofascial pain involves non-steroidal anti-inflammatory drugs and certain types of anti-depressants known as tricyclic anti-depressants, or TCAs. Procedures performed on trigger points include passive stretching after applying vapo-coolant or injection of the trigger points with local anesthetics and sometimes steroid. When symptoms are resistant to such management, epidural steroid injections or specific nerve blocks can be considered. Home remedies include passive stretching while taking a hot shower and applying moist hot packs.
Torticollis is a severe contracture of neck muscles that typically results in the head being painfully twisted to one side with the chin pointing to the opposite side. This pattern is secondary to the involvement of the SCM, or sternocleidomastoid muscle, one of the two most commonly involved muscles in the neck and upper back. Torticollis can be congenital (present at birth) or secondary to injury to the muscles and tissues of the neck. It can also be the result of disease to the central nervous system. Torticollis may result in permanent contracture of the neck muscles.
In trying to classify torticollis, your physician may order x-rays and if there is a specific neurologic deficit associated with the condition, an MRI or CT scan may be warranted.
Spasmodic torticollis can be treated with medications known as anticholinergics. Valium has also been used. Haldol has also been used for more severe cases.
The two most common muscles involved in this condition, the SCM and the trapezius muscles, share innervation by the spinal accessory nerve. Blocking this nerve can improve symptoms in many instances. The muscles themselves may also be injected directly with local anesthetic. Other nerve blocks and trigger point injections may be necessary if additional muscles are involved. Injections and nerve blocks are coupled with physical therapy to enhance recovery. For severe cases that are resistant to such therapeutic maneuvers, spinal cord stimulation and specific surgical procedures may be required.
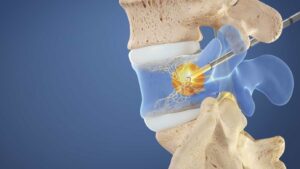
Cervical spondylosis refers to degenerative changes in the joints and intervertebral disks of the cervical spine. These changes occur over time from wear and tear and result in neck pain. Specific changes include dehydration of intervertebral disks resulting in disk bulging, leakage of disk material, inflammation and compression of nerve roots and bone spur formation. Along with nerve roots, the spinal cord itself can be compressed. Ligament and joint hypertrophy or enlargement, can also lead to nerve compression and irritation. The most common nerve roots affected are at C5 and C6 which represents the mid-cervical level.
The neck pain can be poorly localized, exacerbated with movement and be accompanied by muscle spasm. X-rays, MRI or CT scans can assist in the diagnosis by excluding other causes of neck pain such as infection or cancer. Nerve root compression can result in numbness or tingling in the arm and in severe cases, weakness or paralysis of the arm. Treatment includes conservative therapy such as NSAIDS and physical therapy. Cervical epidural steroid injections and other specific nerve blocks may be warranted. Surgery is reserved for cases where significant symptoms such as worsening arm weakness or paralysis develop.
Compression of the cervical spinal cord itself is known as cervical myelopathy. The compression can be secondary to enlarged ligaments, herniated discs, radiation treatment, a diminished blood supply, cancer or infection. While a posterior compression typically results in sensory loss, motor loss and weakness can result from an anterior compression. The spinal cord compression can initially be painless but can result in foot numbness and unsteadiness while walking.
For patients with cervical myelopathy with radicular symptoms of less than one month in duration with no significant finding on x-ray, MRI or CT scan, conservative treatment with a soft collar and non-steroidal anti-inflammatory drugs is indicated. For symptoms lasting more than a month in duration, cervical isometric exercise, trans-cutaneous electrical nerve stimulation, anti-depressants, anticonvulsants, muscle relaxants and cold or hot packs are indicated.
In cervical myelopathy that results from spondylosis, spinal stenosis, herniated disc(s), arthritis or myofascial pain, cervical epidural steroid injections have found to be effective. Surgery is reserved for worsening neurologic deficits along with significant cord compression.
Facet joints are the connections between the vertebral bodies of the spinal canal. They provide structural support to the spinal column and allow limited motion. Cervical facet joint disease can cause localized symptoms or radicular/radiating pain. It can be difficult to differentiate from disk disease and can often occur with disk disease. Facet arthropathy can arise from acute injury but most commonly occurs secondary to chronic changes in the facet joints brought on by disk degeneration, spondylosis, repetitive stress and strain and weight bearing.
Cervical facet joint irritation may be associated with muscle spasms and headaches. Facet joint symptoms may also be like those of cervical disk nerve root irritation resulting in neck pain and radiating pain to the shoulders and arms. Cervical facet joint disease can occur concomitantly with nerve root irritation caused by cervical disk disease.
Extending or rotating the neck stresses the facet joints and reproduces the symptoms. Tenderness is often present when the area above the facet joints is pressed. X-ray, CT and MRI scans may show abnormalities of the facet joints.
Initial treatment of facet symptoms is conservative. Nonsteroidal anti-inflammatory drugs, tricyclic antidepressants, physical therapy and transcutaneous electrical nerve stimulation may afford relief. Facet joint injections with local anesthetic and steroid may be beneficial if conservative therapies fail. Injections should only be attempted if the symptoms can be supported by the findings on imaging studies.
If the injections provide only temporary relief of symptoms, ablation of the nerve supply to the joints can be achieved with radiofrequency techniques, thermocoagulation or phenol injection. Severe cases can be treated with surgical techniques such as cervical fusion with bone graft or spinal hardware/implants.
In summary, causes of neck pain can vary from short lived conditions that are simple to manage and treat to serious and even life threatening states that require immediate intervention by specialty physicians. Neck pain can involve other parts of the upper body such as the head, shoulders, upper back and arms. Appropriate diagnosis by a physician trained to manage such conditions, along with the appropriate diagnostics studies such as MRI can help determine the underlying cause or causes. Most cases of neck pain can be managed conservatively but a good number may require interventional procedures. Some may require surgery.