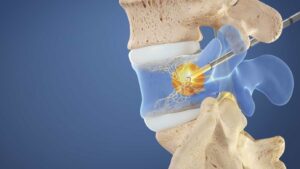
A pinched nerve typically refers to nerve compression due to a variety of factors. Local degenerative changes in or near the spinal column involving intervertebral discs, facet joints and ligaments can cause nerve root compression. These can be due to disc bulges or herniations, facet hypertrophy, ligament hypertrophy, osteochondral spurs or spondylolisthesis or slippage of a one vertebral body over another.
Pinched nerves can occur anywhere in the body where nerves travel through bony and ligamentous structures. Some of the most common sites of nerve compression are the neck and the lower back.
“Pinched Nerve” or nerve compression is typically diagnosed by a physician or chiropractor after careful history taking from the patient. This is followed by a physical exam where the pain may be reproduced after certain motions. A physician may order additional studies such as an MRI to look for pathologic changes in or near the spine that may be causing the nerve compression.
Nerve root compression symptoms typically include pain, inflammation and often shooting pain down the arm or leg. Treatment includes conservative measures such as over-the-counter pain relievers, rest and physical therapy. Most cases have symptomatic resolution over time and only conservative treatment measures are needed.
If pinched nerve symptoms persist after conservative therapy, interventional pain management injections may be warranted. These are typically performed under fluoroscopy which is a “live” x-ray. It allows the physician to see bone and some other anatomical structures in different “frames” while performing a procedures or surgery.
The most common interventional pain management procedures for nerve root compression near the spine is called a selective nerve root block. During this procedure, the physician guides a fine needle under fluoroscopy near the pinched nerve. The fluoroscopy helps the physician guide the needle close to the nerve compression while avoiding anatomical structures that might be damaged if penetrated by the tip of the needle. Once the tip of the needle is close to the nerve root compression, steroid is injected next to the pinched nerve but not into the nerve. The purpose of the steroid is to decrease inflammation and improve symptoms. If symptoms do not resolve, the procedure can be repeated. Typically, it is repeated up to two times with each procedure separated by a time interval of two weeks.
If symptoms are severe to the point where the nerve root compression causes unbearable, unremitting pain, neurological symptoms such as arm or leg weakness or in the case of a pinched nerve in the lower back, loss of bowel or bladder control, surgery is the preferred intervention.
The most common spinal decompressive surgery has traditionally been microdiscectomy. It is considered a minimally invasive surgery in which the herniated intervertebral disc fragments that are causing the nerve root compression are removed. A newer, even less invasive technique involves using a narrow, hollow tube through which instruments are passed to remove the disc fragments. Visualization during this “endoscopic” surgical procedure is aided by a digital camera positioned on the end of the instrument along with a light source. This technique is meant to minimize the surgical trauma to the patient, reduce the incidence of complications and to shorten the recovery time.
Interventional pain management procedures such as selective nerve root block and surgical procedures such as microdiscectomy for pinched nerves are typically followed by a course of physical therapy in order to assist in the patient’s recovery and allow her/him to get back to their daily routine.